Member LoginDividend CushionValue Trap
|
The Curious Cases of Intuitive Surgical and Teva Pharma: What We Have Learned
publication date: Nov 1, 2013
|
author/source: Brian Nelson, CFA
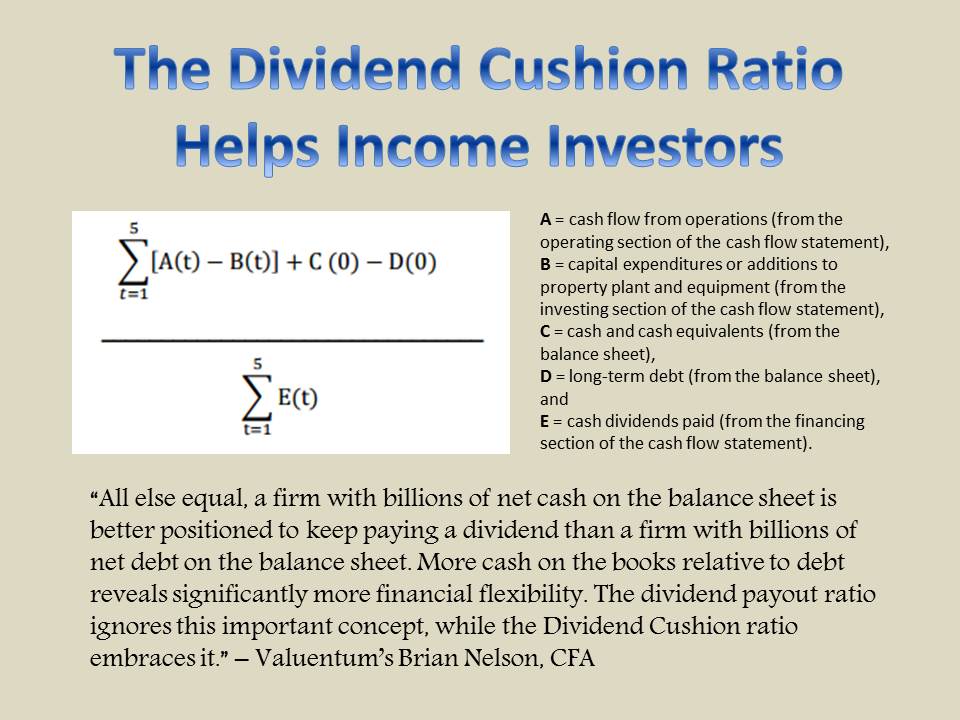
Within every portfolio, there will be a couple companies that do not live up to immediate expectations. Two such companies in our Best Ideas portfolio that haven’t yet delivered on our theses are Intuitive Surgical (ISRG) and Teva Pharma (TEVA). We hold the Healthcare Select SPDR ETF (XLV) in the Best Ideas portfolio as well (it has been a top performer) and our healthcare picks—Johnson & Johnson (JNJ) and Medtronic (MDT)—have performed wonderfully in our Dividend Growth portfolio, but we’re still waiting for our theses to be confirmed with respect to Intuitive Surgical and Teva Pharma. Before we go any further, however, we think it is important to reiterate that the size of the weighting of a position in our actively-managed portfolios indicates the conviction we have in the idea. For example, our portfolio weightings in Intuitive Surgical and Teva Pharma are 1.7% and 1.9%, respectively. By comparison, our weightings in Apple (AAPL) and Ford (F), for example, are nearly 7%, suggesting we like the latter two ideas several times more than the former two ideas. The size of the weighting in our actively-managed portfolios tells you just how confident we are in the idea relative to others. With respect to Intuitive Surgical and Teva Pharma, new pieces of information came to light after we had established our position in each company. Intuitive Surgical: Blindsided by ACOG President’s Aggressive Comments For Intuitive Surgical, it was the extreme negative publicity mid-March following a publication posted by American Congress of OB/GYN (ACOG) President James T. Breeden, MD. We were quite surprised with how passionate the president was against robotic surgery. We show the full publication below: Many women today are hearing about the claimed advantages of robotic surgery for hysterectomy, thanks to widespread marketing and advertising. Robotic surgery is not the only or the best minimally invasive approach for hysterectomy. Nor is it the most cost-efficient. It is important to separate the marketing hype from the reality when considering the best surgical approach for hysterectomies. The outcome of any surgery is directly associated with the surgeon’s skill. Highly skilled surgeons attain expertise through years of training and experience. Studies show there is a learning curve with new surgical technologies, during which there is an increased complication rate. Expertise with robotic hysterectomy is limited and varies widely among both hospitals and surgeons. While there may be some advantages to the use of robotics in complex hysterectomies, especially for cancer operations that require extensive surgery and removal of lymph nodes, studies have shown that adding this expensive technology for routine surgical care does not improve patient outcomes. Consequently, there is no good data proving that robotic hysterectomy is even as good as—let alone better—than existing, and far less costly, minimally invasive alternatives. Vaginal hysterectomy, performed through a small opening at the top of the vagina without any abdominal incisions, is the least invasive and least expensive option. Based on its well-documented advantages and low complication rates, this is the procedure of choice whenever technically feasible. When this approach is not possible, laparoscopic hysterectomy is the second least invasive and costly option for patients. Robotic hysterectomy generally provides women with a shorter hospitalization, less discomfort, and a faster return to full recovery compared with the traditional total abdominal hysterectomy (TAH) which requires a large incision. However, both vaginal and laparoscopic approaches also require fewer days of hospitalization and a far shorter recovery than TAH. These two established methods also have proven track records for outstanding patient outcomes and cost efficiencies. At a time when there is a demand for more fiscal responsibility and transparency in health care, the use of expensive medical technology should be questioned when less-costly alternatives provide equal or better patient outcomes. Hysterectomy is one of the most common major surgeries in the US and costs our health care system more than $5 billion a year. At a price of more than $1.7 million per robot, $125,000 in annual maintenance costs, and up to $2,000 per surgery for the cost of single-use instruments, robotic surgery is the most expensive approach. A recent Journal of the American Medical Association study found that the percentage of hysterectomies performed robotically has jumped from less than 0.5% to nearly 10% over the past three years. A study of over 264,000 hysterectomy patients in 441 hospitals also found that robotics added an average of $2,000 per procedure without any demonstrable benefit. If most women undergoing hysterectomy for benign conditions each year chose a vaginal or laparoscopic procedure—rather than TAH or robotic hysterectomy—performed by skilled and experienced surgeons, pain and recovery times would be reduced while providing dramatic savings to our health care system. Conversely, an estimated $960 million to $1.9 billion will be added to the health care system if robotic surgery is used for all hysterectomies each year. Aggressive direct-to-consumer marketing of the latest medical technologies may mislead the public into believing that they are the best choice. Our patients deserve and need factual information about all of their treatment options, including costs, so that they can make truly informed health care decisions. Patients should be advised that robotic hysterectomy is best used for unusual and complex clinical conditions in which improved outcomes over standard minimally invasive approaches have been demonstrated. Frankly, we were blindsided. When someone of this industry authority presents a case against continued product adoption of robotic surgery, it will cause a hiccup in demand whether the comments are biased or not. Our view is that President Breeden was speaking more to a constituency than as a medical professional with hard facts, indirectly flattering doctors at times: “the outcome of any surgery is directly associated with the surgeon’s skill.” We also picked up a ‘resistance to change’ disposition in his comments: “studies show there is a learning curve with new surgical technologies, during which there is an increased complication rate. Expertise with robotic hysterectomy is limited and varies widely among both hospitals and surgeons.” Breeden’s appeal to a constituency—where the majority may not yet be experts on robotic hysterectomy—lead us to believe that not all comments may be free from bias. A ‘learning curve,’ for example, should not be relevant as an impediment to a product’s long-term adoption, if its efficacy is documented in many instances, as Breeden outlined: “while there may be some advantages to the use of robotics in complex hysterectomies, especially for cancer operations that require extensive surgery and removal of lymph nodes…; robotic hysterectomy generally provides women with a shorter hospitalization, less discomfort, and a faster return to full recovery compared with the traditional total abdominal hysterectomy (TAH) which requires a large incision…; patients should be advised that robotic hysterectomy is best used for unusual and complex clinical conditions in which improved outcomes over standard minimally invasive approaches have been demonstrated.” The slowdown in orders for the da Vinci has certainly materialized since President Breeden’s publication, but we think there’s enough positive substance in the president’s comments that suggests robotic surgery still has a long runway of future growth. With Intuitive Surgical pumping more and more money into research and development (it invested $170 million in 2012), we think it is just a matter of time before the firm is able to make the cost decision a very easy one for hospitals. Though unlikely given the tone of the publication, it’s possible that President Breeden was simply calling on Intuitive Surgical to become more efficient (and using his constituency to enact change). For one, we do find it quite unusual that the idea of making robotic surgery less expensive wasn’t even mentioned. The publication simply tried to counter the adoption of robotic surgery, without even acknowledging the ability of Intuitive Surgical to use pricing to attract more placements (and lower the cost equation for hospitals). Investors should continue to expect a highly-volatile stock and a flurry of contradictory information with respect to Intuitive Surgical’s products in coming weeks, months, and years. However, it is our view that robotic surgery is here to stay, and the potential for Intuitive Surgical to make in-roads into other robotic surgery applications is an open-ended opportunity not appropriately captured in its market price. The recent slowdown in da Vinci orders may just be the catalyst that creates another breakthrough product at the firm. Takeaway: It’s likely that investors may see Intuitive Surgical’s shares at $200 before they hit $600 again, but the long-term is still bright. Shares are down about 20% from our cost basis. << Clinical Evidence, per Intuitive Surgical Teva: Copaxone Disappointment; Management Controversy The fundamental path of Teva was equally surprising. Shortly after we established a position, the hurdles with respect to its multiple-sclerosis drug Copaxone (which accounts for roughly half of profits) became even greater: “The U.S Federal Court of Appeals confirmed validity of select COPAXONE patents through May 2014, but not others including one patent expiring September 2015. We are disappointed with this part of the Appeals Court decision and we will appeal that decision. I want to remind you that COPAXONE is a complex synthetic peptide. We believe that a purported generic version would need full scale, placebo-controlled clinical trials in RRMS patients. As a consequence, we are not sure of a generic timing or approval. In addition to appealing the court's decision, this company has been preparing for the potential launch of the generic COPAXONE. In May 2013, the U.S. FDA accepted our submission for a more convenient schedule of three times weekly dosing of COPAXONE, 40 milligrams per meal. We anticipate FDA actions in the first quarter of 2014, and if approved we are prepared with an aggressive launch strategy for the first half of 2014.” The patent expiration of its current large profit-driver Capaxone in May 2014 is roughly a full year earlier than what we had been expecting prior to initiating our position in the firm in our Best Ideas portfolio. Then, we were blindsided again. Just this week, CEO Jeremy Levin stepped down as CEO – the day before the firm released third-quarter results. Certainly, this management change was not anticipated, and while the firm’s quarterly performance wasn’t bad, the abrupt exit by CEO Levin does bring into question the firm’s long-term strategy. Still, Teva’s global generic opportunity is arguably the best within our coverage universe, and we’re excited about its NTE pipeline, which we’re expecting to be a multi-billion dollar revenue stream in coming years. The company is uniquely-positioned to capture the NTE opportunity because of the firm’s ability to combine its generic and branded-drug expertise across indications. Investors should fully expect the next 12-24 months to be difficult for the company with respect to year-over-year comparisons, but we still feel comfortable holding shares in the portfolio of our Best Ideas Newsletter. The long-term opportunity for lower-cost generics in an environment where governments across the globe are looking to cut expenses and become more efficient is just too great to pass up, in our view. Takeaway: Losing close to half of its profits in coming years as a result of losing exclusivity on Copaxone will translate into some tough sledding for Teva Pharma investors. However, we still believe the long-term is bright. Valuentum’s Take: What We’ve Learned With respect to Intuitive Surgical, we became so enamored with the long-term prospects of robotic surgery that we were just too flexible with our entry point. The firm’s Valuentum Buying Index rating was a 5 when it entered our Best Ideas portfolio. We intend to better follow our own methodology and don’t intend to make a leap just to gain exposure to a long-term story without substantial VBI support first. This is a process error on our part. With respect to Teva Pharma, the appeal of the long term was a contributing factor, too. Though we added the firm to the portfolio with a VBI rating of 6, Teva has registered a 9 in the past. Interestingly, we think Teva Pharma is an example of the strength of our methodology. In a situation where the firm will lose more than half of profits in coming years and where a controversial and unexpected change in the executive suite occurred, shares are down a meager 8%. We believe Teva highlights the positive risk/reward profile of firms that register a 9 or 10 on the VBI. When things go unexpectedly and incredibly wrong, stocks with VBI ratings of 9 and 10 remain very resilient. |